The differential diagnosis in pediatric lymphadenopathy includes bacterial, viral, fungal, and idiopathic causes. A systematic approach to patient evaluation is necessary because the differential diagnosis, presentation, and work up must consider infectious, immunologic, neoplastic, and idiopathic disorders. A thorough history and examination are vital to determining the diagnosis and ruling out a malignant process.
Key points
- •
The differential diagnosis in pediatric lymphadenopathy includes bacterial, viral, fungal, and idiopathic causes.
- •
A systematic approach to patient evaluation must be used because the differential diagnosis, presentation, and work up must consider infectious, immunologic, neoplastic, and idiopathic disorders.
- •
A thorough history and physical are vital to determining the diagnosis and ruling out a malignant process.
| CGD | Chronic granulomatous disease |
| CHS | Chédiak-Higashi syndrome |
| CSD | Cat-scratch disease |
| CXR | Chest radiograph |
| EBV | Epstein-Barr virus |
| FNA | Fine-needle aspiration |
| HAART | Highly active antiretroviral therapy |
| IM | Infectious mononucleosis |
| MRSA | Methicillin-resistant Staphylococcus aureus |
| NTM | Nontuberculous mycobacteria |
| PCR | Polymerase chain reaction |
| PPD | Purified protein derivative |
| US | Ultrasound |
Introduction
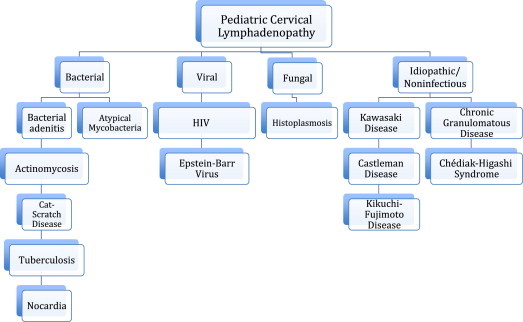
Pediatric cervical adenopathy is a frequently encountered clinical concern that often presents to an otolaryngologist. A systematic approach to the evaluation of these patients must be used because the differential diagnosis, presentation, and work up must consider infectious, immunologic, neoplastic, and idiopathic disorders ( Fig. 1 ). The assessment and diagnosis hinge on a thorough physical examination, the decision for laboratory data, and necessary imaging. A complete history, including recent travel, ethnicity, and other social dynamics, may influence exposure to different pathogens. A detailed history, physical examination, laboratory assessment, and appropriate radiologic examinations can often identify the disease process before the need for surgical intervention.
Introduction
Pediatric cervical adenopathy is a frequently encountered clinical concern that often presents to an otolaryngologist. A systematic approach to the evaluation of these patients must be used because the differential diagnosis, presentation, and work up must consider infectious, immunologic, neoplastic, and idiopathic disorders ( Fig. 1 ). The assessment and diagnosis hinge on a thorough physical examination, the decision for laboratory data, and necessary imaging. A complete history, including recent travel, ethnicity, and other social dynamics, may influence exposure to different pathogens. A detailed history, physical examination, laboratory assessment, and appropriate radiologic examinations can often identify the disease process before the need for surgical intervention.
Bacterial
Bacterial Cervical Lymphadenitis
Recent reports have identified an increased incidence of pediatric deep neck infections. The increase in methicillin-resistant Staphylococcus aureus (MRSA) has played a role in the increasing prevalence of this disease. S aureus is cultured from pediatric neck abscesses in up to 60% of the cases; 22% to 29% are MRSA. Although reactive lymphadenopathy is commonly in response to upper respiratory illnesses, the duration and severity of these infections is usually short lived.
Clinical presentation
Presentation typically involves neck mass, fever, cervical lymphadenopathy, poor oral intake, and neck stiffness. Coticchia and colleagues found that children younger than 4 years with bacterial cervical lymphadenitis had a higher incidence of agitation, cough, drooling, lethargy, palatal or pharyngeal swelling, respiratory distress, retractions, rhinorrhea, and stridor than children older than 4 years.
Diagnosis
Diagnosis can be made clinically, although is usually supported by imaging that includes ultrasound (US) or CT. Imaging modalities may aid in revealing characteristics consistent with an infected congenital anomaly such as a branchial cleft cyst or a thyroglossal duct cyst. Common pathogens include streptococcus and staphylococcus species, which can account for up to 80% of cultures.
Management
Up to 90% to 100% of community-acquired MRSA is sensitive to clindamycin and trimethoprim-sulfamethoxazole. Nosocomial strains of MRSA may have a resistance to these 2 antibiotics at a rate of up to 10% to 20% and is universally resistant to erythromycin. Treatment involves broad-spectrum (with gram-positive and gram-negative coverage) oral or intravenous antibiotics with surgical intervention reserved for those with frank abscess formation seen on imaging or failure of medical management. Increasing antibiotic resistance plays a role in empiric antibiotic therapy because up to 18% of methicillin-sensitive S aureus is resistant to clindamycin. Cabrera and colleagues retrospectively reviewed 89 children with head and neck infections and the most common bacteria isolated was group B streptococcus. Age seems to be a determining factor in the bacterial type because children less than age 1 year are more likely to have S aureus as the infecting organism.
Infection progression
Often, when these infections progress to suppuration, surgical intervention is required because complications of this this process can include
- •
Airway obstruction
- •
Internal jugular vein thrombosis
- •
Neurologic defects
- •
Carotid blowout
- •
Death
Adenitis may spread and seed adjacent deep cervical spaces such as the retropharyngeal space, parapharyngeal space, or submandibular space. The retropharyngeal space lies posterior to the buccopharyngeal fascia and may be synonymous with the prevertebral space. A transoral approach is used for incision and drainage of this area. The parapharyngeal space lies lateral to the buccopharyngeal fascia and medial to the pterygoid muscle and parotid gland and may be approached via a transoral or external transcervical approach. The submandibular space, which runs from the hyoid bone to the mandible, is also approached via an external transcervical approach.
Actinomycosis
Actinomycosis is a progressive granulomatous infection characterized by abscesses, draining sinuses, and fibrosis of tissues. The pathogens are fermentative organisms, including Actinomyces , Propionibacterium , and Bifidobacterium . Gram-positive, diphtheroid Actinomyces species produces most of the infections. The most commonly affected site is the cervicofacial location. Many sites may become affected by the infection, including thorax, pelvis, and central nervous system, which can lead to spinal cord compression. Actinomycosis is a fastidious bacteria, evident because it requires enriched culture media at 37°C to grow and must be aided by 6% to 10% ambient carbon dioxide. Growth can be detected between 3 and 21 days. Of note, Nocardia and Actinomyces are clinically indistinguishable on gram stain although Nocardia is aerobic and partially acid-fast. These organisms live as endosaprophytes in dental caries, tonsillar crypts, and in the gingiva with no environmental reservoir. Patients presenting with poor dental hygiene along with extensive cervical lymphadenopathy should be evaluated for Actinomycosis .
Clinical presentation
Presentation of an Actinomycosis infection can occur at any age. In the pediatric population it occurs with dental caries and lymphadenopathy at the angle of the mandible or in the submandibular region. Acutely, this can present as cellulitic change in the overlying skin with edema and pain. The chronic form of the disease can present as chronic inflammation and induration, and progress to multiple abscesses with draining sinus tracts, of which 25% contain sulfur granules. Presentation can include low-grade fever and enlargement of locoregional cervical lymph nodes but can also become more extensive and include osteomyelitis.
Diagnosis
Diagnosis is based on culture results of incisional or excisional biopsy, or fine-needle aspiration (FNA) samples with multiple biopsies at different levels recommended to enhance possibly of diagnosis. CT or MRI can be used to evaluate this area with the common findings of an enhancing soft tissue mass with an low attenuating center with adjacent soft tissue inflammation. An actinomycosis infection in a child indicates the need for evaluation for an underlying immunologic deficiency such as chronic granulomatous disease (CGD).
Management
The treatment choice is penicillin G (50–75 mg/kg/d intravenously in 4 daily divided doses) for 4 to 6 weeks. This may be followed by oral penicillin V (30–60 mg/kg/d administered in 4 divided doses) for 2 to 12 months. Tetracycline can be used for patients who are allergic to penicillin; however, it can cause dental staining. Duration of therapy depends on disease burden, sites of infection, and radiologic and clinical response to therapy. Medical therapy alone may be adequate for treatment but adjuvant surgical debridement may also be indicated. Surgical therapy, although not curative alone, is indicated for curettage of bone, resection of necrotic tissue, excision of sinus tracts, and drainage of soft tissue abscesses.
Cat-Scratch Disease
The frequent occurrence of cat-scratch disease (CSD) with associated cervical lymphadenopathy makes this one of the most common causes of infectious cervical lymphadenopathy. The incidence of this in the Unites States is 9.3 per 100,000. The pathogen is the gram-negative bacteria Bartonella henselae . Kittens are the reservoir for this bacterium. Infections typically involve children and adolescents younger than 18 years old with boys and girls equally affected. After a scratch or bite, the typical presentation usually begins as erythema, papules, or pustules occurring at the scratch line with adenopathy in the affected region 2 to 3 weeks after the incident and may remain up to 6 months in 20% of patients.
Clinical presentation
Patients may present with general malaise, headache, and fever; however, the most common clinical manifestations range from painless lymphadenopathy not involving the overlying skin to large cervical abscesses. After upper-extremity adenopathy, head and neck presentation is the second most common site. Cervical and submandibular nodes make up most of the sites affected, followed by preauricular or parotid involvement.
Diagnosis
Diagnosis is based on biopsy or serologic testing. Previously, diagnosis was clinical and based on history of contact with a kitten, positive CSD skin test, regional lymphadenopathy in which other causes have been ruled out, and an excisional lymph node biopsy with histopathologic findings of CSD. Warthin-Starry silver staining is used to visualize pleomorphic bacilli in the walls of blood vessels and in microabscesses. Bacilli may stain positive by Warthin-Starry staining early in the disease process but is rarely detected later in the disease. On excisional biopsy in the early stage of the disease, reactive lymphoid hyperplasia develops, whereas later in the course of the disease granuloma formation and microabscesses may form. Serologic testing consists of IgG and IgM antibodies, with IgM antibodies the most sensitive. If negative, polymerase chain reaction (PCR) detection of Bartonella DNA is used on biopsy material. Both granulomas and abscesses may be found in the same specimen. The resultant lymphadenopathy enlarges and may not resolve for 2 or 3 months.
Management
Treatment is usually supportive but definitive diagnosis must be ascertained before observation. Signs of systemic disease, which may be seen in immune-compromised hosts, can include endocarditis, osteolytic lesions, and meningoencephalitis. Systemic symptoms warrant treatment consisting of ciprofloxacin, erythromycin, rifampin, or gentamycin.
Nocardia
Nocardia is found in soil around the world and commonly presents as neck adenopathy in immunocompromised individuals; it can be associated with disseminated disease.
Diagnosis
Diagnosis remains difficult unless there is a high level of suspicion for this process as the primary symptom is a painless neck mass. The organism is very slow growing and biopsy must be obtained to obtain tissue for diagnosis. Nocardia infections diagnosed in children require further work-up for an underlying immunodeficiency.
Management
The treatment choices for Nocardia infections are: trimethoprim-sulfamethoxazole, imipenem, amikacin, and linezolid. Boiron and colleagues reviewed nocardial infections from 1987 to 1990 and determined that recent treatment with corticosteroids represented a significant factor for increased mortality from these infections.
Nontuberculous Mycobacteria
Nontuberculous mycobacteria (NTM) infection also commonly presents with cervical lymphadenopathy in children. These ubiquitous organisms are seen in the soil but can also be found in water, milk, and domestic animals. Organisms that cause NTM typically include Mycobacterium intracellulare complex, M scrofulaceum , and M kansasii .
Clinical presentation
The typical presentation is a painless neck mass seen in an immunocompetent child that has been unresponsive to standard antibiotics. This can be associated with skin discoloration, including erythema or a violaceous discoloration, and, less often, fistula formation. This occurs most often in female patients and children younger than 5 years old. These lesions are slow growing but a late complication is fistulization and drainage. Infection commonly involves the submandibular and cervical area and upper cervical area and often presents with parotid involvement ( Figs. 2 and 3 ).

Diagnosis
Diagnosis is based on purified protein derivative (PPD) intradermal testing or on cultured tissue and PCR testing for mycobacterial RNA from biopsy (excisional or FNA). Imaging usually involves US, CT, or MRI. Findings on these studies are nonspecific but can consist of solid hypoechoic masses that can appear hypodense on CT. Histopathologic results reveal chronic granulomatous inflammation with areas of caseous necrosis.
Management
Treatment usually involves an oral antibiotic regimen consisting of rifampin and clarithromycin. If this fails, surgical excision or curettage can be used as an alternative approach to reduce the burden of disease. If surgical excision is planned, the technique involves removing that total mass en bloc with any involved skin or adjacent tissue, closing the skin to prevent fistula formation. When adherence to facial nerve is encountered or tissue involvement is extensive, a wait-and-see approach can be considered with adjuvant oral antimycobacterial antibiotics. Recent studies have suggested that observation, with or without antibiotic therapy, often can lead to resolution of 6 months to 1 year. Some investigators have postulated that the depth of cervical disease helps determine outcome, whereas disease deeper to the sternocleidomastoid muscle was more likely to require no intervention and resolve without morbidity.
Tuberculosis Lymphadenitis
Tuberculosis is a chronic air-borne infectious disease caused by M tuberculosis . Nearly 2 billion people are affected by this disease globally. High-risk groups include the immunocompromised, elderly, healthcare workers, and immigrants.
Clinical presentation
Individuals infected typically have pulmonary hilar and cervical lymphadenopathy that is commonly bilateral. This typically indicates hematogenous spread from pulmonary disease. Cervical lymphadenopathy can be part of the primary infection or secondary (organ) tuberculosis. Early-phase lymphadenitis is characterized by a nontender, firm lymph node, which develops caseous necrosis and softens into an abscess.
Diagnosis
Screening for this disease process is based on a positive PPD. Other diagnostic tests may include chest radiograph (CXR) and excisional biopsy or FNA of cervical lymph node with PCR testing. Ziehl-Neelsen staining of obtained tissue occasionally shows short rod-shaped bacteria in the coagulation necrosis. Histology is characterized by central caseous necrosis surrounded by an epithelioid cell layer and sporadic Langerhans giant cells.
Management
Healing occurs with calcification of the affected node. Treatment consists of isolation of a patient with active disease along with a multidrug antitubercular regimen. Incision and drainage of cervical lymphadenopathy should be avoided because there is concern for fistulization.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


