Salivary gland neoplasms are rare in children. In infants most tumors are benign hemangiomas, with some notable exceptions, such as sialoblastomas. An asymptomatic swelling in the periauricular region is the most common presenting complaint in older children. Approximately 50% of these lesions are malignant, which dictates a thorough diagnostic evaluation by a head and neck surgeon. Surgical excision is the primary treatment modality. Prognosis is primarily determined by histopathologic findings. This review discusses neoplastic lesions of the salivary glands in children, and malignant epithelial tumors in particular.
Key points
- •
Salivary gland neoplasms are rare in children.
- •
An asymptomatic swelling in the periauricular region is the most common presenting complaint in older children.
- •
Approximately 50% of salivary gland lesions are malignant, dictating a thorough diagnostic evaluation by a head and neck surgeon.
- •
Surgical excision is the primary treatment of lesions.
- •
Histopathologic findings determine prognosis.
Introduction
Disorders of the salivary glands can be broadly divided into neoplastic and nonneoplastic disease. Further divisions can be made, as salivary gland lesions are associated with a wide spectrum of etiology ( Table 1 ). The age of the patient narrows the potential diagnoses, with vascular lesion often presenting at birth or within the first year of life, whereas solid tumors, with notable exceptions, are more likely to occur in older children. Inflammatory disease usually has a relatively rapid onset in contrast to neoplastic or congenital processes, which have more insidious onsets. Tenderness of the affected area is most often associated with inflammatory disease. Persistent, firm, painless, well-circumscribed lesions should be thoroughly investigated with imaging such as ultrasonography, computed tomography (CT), and MRI, and occasionally with fine-needle aspiration in older children. In a large review of 9993 salivary gland lesions, 430 were in children, accounting for 4.3% of the total. Of the lesions in children, 262 were nonneoplastic and 168 others were considered tumors. This review discusses neoplastic lesions of the salivary glands in children, and malignant epithelial tumors in particular.
| Nonneoplastic lesions | |
| Congenital/developmental | First branchial arch anomalies |
| Inflammatory and infection | Acute bacterial sialadenitis |
| Viral: mumps, cytomegalovirus, Coxsackie A or B, or parainfluenza virus | |
| Human immunodeficiency virus (HIV)-associated salivary glands | |
| Recurrent parotitis in children (RPC) | |
| Granulomatous disease | Mycobacterial disease |
| Actinomycosis | |
| Sarcoidosis | |
| Necrotizing sialometaplasia | |
| Autoimmune | Sjögren syndrome |
| Cysts | Ranula |
| Mucocele | |
| Neoplastic tumors | |
| Benign epithelial | Pleomorphic adenoma |
| Benign mesenchymal | Hemangioma |
| Lymphangioma | |
| Malignant-epithelial | Mucoepidermoid carcinoma |
| Acinic cell carcinoma | |
| Adenoid cystic carcinoma | |
| Sialoblastoma | |
| Mesenchymal | Rhabdomyosarcoma |
Introduction
Disorders of the salivary glands can be broadly divided into neoplastic and nonneoplastic disease. Further divisions can be made, as salivary gland lesions are associated with a wide spectrum of etiology ( Table 1 ). The age of the patient narrows the potential diagnoses, with vascular lesion often presenting at birth or within the first year of life, whereas solid tumors, with notable exceptions, are more likely to occur in older children. Inflammatory disease usually has a relatively rapid onset in contrast to neoplastic or congenital processes, which have more insidious onsets. Tenderness of the affected area is most often associated with inflammatory disease. Persistent, firm, painless, well-circumscribed lesions should be thoroughly investigated with imaging such as ultrasonography, computed tomography (CT), and MRI, and occasionally with fine-needle aspiration in older children. In a large review of 9993 salivary gland lesions, 430 were in children, accounting for 4.3% of the total. Of the lesions in children, 262 were nonneoplastic and 168 others were considered tumors. This review discusses neoplastic lesions of the salivary glands in children, and malignant epithelial tumors in particular.
| Nonneoplastic lesions | |
| Congenital/developmental | First branchial arch anomalies |
| Inflammatory and infection | Acute bacterial sialadenitis |
| Viral: mumps, cytomegalovirus, Coxsackie A or B, or parainfluenza virus | |
| Human immunodeficiency virus (HIV)-associated salivary glands | |
| Recurrent parotitis in children (RPC) | |
| Granulomatous disease | Mycobacterial disease |
| Actinomycosis | |
| Sarcoidosis | |
| Necrotizing sialometaplasia | |
| Autoimmune | Sjögren syndrome |
| Cysts | Ranula |
| Mucocele | |
| Neoplastic tumors | |
| Benign epithelial | Pleomorphic adenoma |
| Benign mesenchymal | Hemangioma |
| Lymphangioma | |
| Malignant-epithelial | Mucoepidermoid carcinoma |
| Acinic cell carcinoma | |
| Adenoid cystic carcinoma | |
| Sialoblastoma | |
| Mesenchymal | Rhabdomyosarcoma |
Neoplastic tumors
Benign Epithelial Tumors
Pleomorphic adenoma
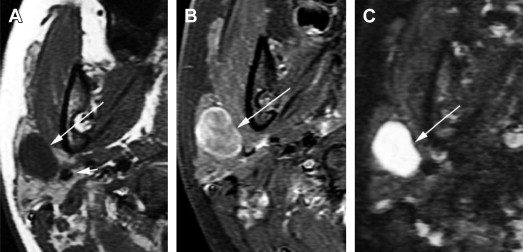
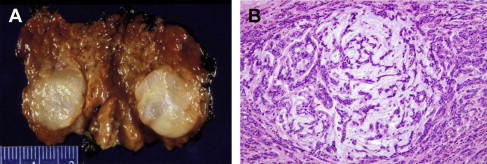
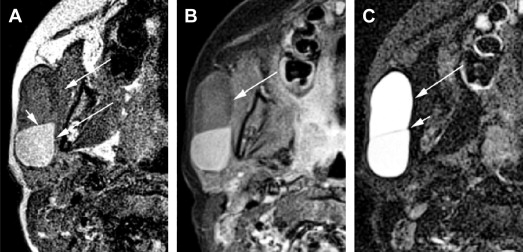
Pleomorphic adenomas (PAs) account for approximately half of all epithelial tumors of the salivary glands and more than 90% of benign salivary gland epithelial tumors. Composite analysis of several studies reveals that most (62%; range 56%–77%) PAs occur in the parotid gland, with the submandibular gland (26%; range 11%–40%) and the minor salivary glands (12%; range 0%–21%) being less frequent sites of origin. The female to male ratio is approximately 1.4:1. The typical presentation of a PA is a slow-growing, painless, and firm mass with an average duration of symptoms of approximately 12 months. On ultrasonography, CT, and MRI, PAs are most commonly well defined. On CT, small calcifications can be seen and on MRI, PAs are typically very bright on T2-weighted images and show homogeneous or heterogeneous enhancement ( Fig. 1 ). On gross inspection, PAs are well circumscribed and lobulated with a smooth surface. Classic histologic features include epithelial/myoepithelial cells in a myxochondroid matrix ( Fig. 2 ). The relative amounts of cellular and stromal tissue have no bearing on the aggressiveness of the tumor. The preferred treatment of parotid PAs involves superficial parotidectomy or total parotidectomy, depending on lesion location. This approach yields local control rates in excess of 95%. By contrast, the risk of tumor recurrence following lesion enucleation approaches 43%. Although PAs are benign neoplasms, there is potential for malignant transformation. The average incidence of carcinoma ex pleomorphic adenoma is estimated to be 6.2%. The risk of malignant degeneration in an untreated patient seems to be related, in part, to how long the lesion has been present, increasing from approximately 1.5% in the first 5 years to 9.5% for PAs present for longer than 15 years. Carcinomas ex pleomorphic adenoma are rare in children, with only 4 cases identified in the composite review of retrospective series. Long life expectancy, combined with documented recurrences up to 30 years after initial resection, increases the recurrence risk in children, with resultant long-term follow-up being mandatory.
Other benign epithelial tumors
The remaining benign epithelial tumors consist mostly of Warthin tumors and others such as lymphoepitheliomas, myoepitheliomas, and basal cell adenomas. These tumors are exceedingly rare in the pediatric setting, so adult guidelines are generally followed. Treatment involves surgical resection, usually consisting of parotidectomy with preservation of the facial nerve.
Benign Mesenchymal Tumors
Hemangioma
Approximately 30% of hemangiomas are present at birth and the rest arise shortly thereafter. Hemangiomas account for 90% of all salivary tumors in children younger than 1 year. In some series they account for approximately half of all pediatric salivary gland tumors. Hemangiomas undergo a distinct pattern of development, proliferating rapidly during the first 1 to 2 months of life. Often a second growth spurt occurs between 4 and 6 months of age, followed by a slower course of involution, which is generally complete by the first decade of life. With regard to salivary gland hemangiomas, 80% arise in the parotid glands, 18% arise in the submandibular glands, and 2% arise in the minor salivary glands.
Clinical presentation
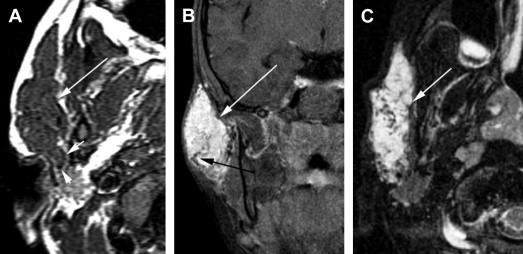
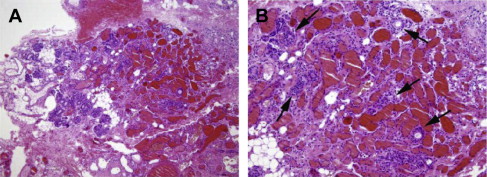
Hemangiomas present as soft, unilateral masses, with or without a bluish discoloration of the skin. Doppler sonography, CT, and MRI can be used to characterize infantile hemangiomas. All imaging modalities show a lobulated, solid, hypervascular mass ( Fig. 3 ). Histologically, hemangiomas are unencapsulated aggregates of closely packed, thin-walled capillaries, usually with endothelial lining. Blood-filled vessels are separated by scant connective tissue ( Fig. 4 ). Treatment is not required unless the lesion is complicated by ulceration or infection, or causes compression of the airway, which occurs more often with segmental hemangiomas. Management choices include sclerotherapy, surgery (parotidectomy), and, more recently, oral propranolol.
Lymphatic malformations
Lymphatic malformations (LMs) are congenital anomalies of the lymphatic system, 90% of which are detected by age 2 years. LMs often present suddenly as a palpable mass related to intralesional hemorrhage or infection. On MRI, LMs are well circumscribed, multicystic, predominantly bright on T2-weighted images, and often show fluid-fluid levels within the cystic components ( Fig. 5 ). Pathologically, LM is a complex of multiple cysts lined with lymphatic vascular endothelium ( Fig. 6 ). Unlike hemangiomas of infancy, LMs do not undergo spontaneous regression. Treatment options consist of sclerotherapy with agents such as OK-432, doxycycline, ethanol, or sodium tetradecyl sulfate 3% for macrocystic lesions, surgery, or combinations of both.
Malignant Epithelial Tumors
Overview
Malignancies of the salivary glands in children and adolescents are exceedingly rare, with an estimated annual incidence of 0.08 per 100,000. Most information on salivary gland neoplasms is derived from retrospective studies conducted at tertiary care oncologic institutions. Approximately 50% of major salivary gland tumors in children are malignant, which is more than twice the proportion reported in the adult population. The most common anatomic site for malignant salivary gland tumors in children is the parotid gland. In one large clinical series :
- •
82% of 315 pediatric epithelial salivary gland malignancies arose within the parotid gland
- •
11% arose within minor salivary glands
- •
7% arose within the submandibular gland
- •
Less than 1% arose within the sublingual gland
Mucoepidermoid carcinoma is by far the most common type of malignant salivary gland tumor in children, accounting for more than 60%. Acinic cell carcinoma (11%) and adenocarcinoma (10%) are also relatively common, whereas adenoid cystic carcinoma (9%), carcinoma ex pleomorphic adenoma (1%) and squamous cell carcinoma (<1%) are comparatively rare.
Epidemiology
Most malignant salivary gland tumors occur in older children and adolescents. One epidemiology study reported an average age of 13.4 years at diagnosis. Benign salivary gland neoplasms, on the other hand, present at a slightly older age (15 years on average). There is a near equal distribution of malignant salivary gland tumors between the sexes.
Clinical presentation
Most commonly, a salivary gland neoplasm presents as a firm mass. As an estimated 50% of these tumors are malignant, a thorough diagnostic evaluation is critical. The average duration a mass is present before clinical presentation is 8 to 12 months. Parotid gland tumors are usually asymptomatic; rarely adenoid cystic and acinar cell carcinomas are painful. Bimanual palpation of submandibular and sublingual masses may reveal fixation of the mass to surrounding structures. The incidence of facial nerve paresis at presentation approaches 4%. Lymphatic metastases are documented at presentation in 3.5% of children.
Diagnosis of salivary gland tumors
Malignant tumors of the minor salivary glands can be challenging to diagnose because of their site-dependent presentation. For example, minor salivary gland malignancies of the hard palate can mimic bone lesions, and those of laryngeal origin may produce airway obstruction, dysphagia, and hoarseness. More than 50% of minor salivary gland malignancies are located within the oral cavity in the pediatric population.
Imaging
Ultrasonography is helpful in distinguishing solid from cystic masses in the salivary glands. In addition, this imaging modality is noninvasive, does not use ionizing radiation, and can often be performed without sedation. Once it has been determined that a parotid or submandibular lesion is solid, more detailed assessment with CT or MRI is recommended. Sedation and radiation considerations may dictate which procedure is initially chosen because in younger children, MRI more commonly requires sedation but does not expose the child to radiation. CT is useful in assessing the size of the lesion, identifying tumor calcifications, defining osseous involvement, and demonstrating lymph node metastases. MRI allows for detailed soft-tissue characterization of the tumor and provides important information in regard to tumor margins, the extent of depth of the lesion, and the pattern of tumoral infiltration into the adjacent parenchyma, and may identify perineural spread. Imaging features strongly suggestive of parotid malignancy are poorly defined tumoral margins with infiltration into the parapharyngeal space and surrounding musculature (see Fig. 1 ; Figs. 7–10 ). Fine-needle aspiration cytology is a diagnostic tool that has a reliable sensitivity and specificity in adults. Although its use in children has some advocates, the role of fine-needle aspiration is controversial, and often requires sedation or general anesthesia in younger children. When undertaken, accuracy can be as low as 33%.
Staging pediatric salivary gland malignancies
For major salivary gland malignancies, the adult TNM staging system is used. For minor salivary gland malignancies the staging system for squamous cell carcinomas, which is tumor-site dependent, is used. Children are often diagnosed at an earlier stage than adults. There is no single grading system for salivary gland cancers. Certain cancers are considered low grade (eg, basal cell adenocarcinoma and acinic cell adenocarcinoma) and others high grade (eg, squamous cell carcinoma and undifferentiated carcinoma). Salivary gland malignancies can also be stratified into low-risk and high-risk tumors, with low-risk tumors being those that do not require treatment beyond excision. The caveat is that high-grade versions of “intrinsically” low-grade tumors exist, as do low-grade versions of typically high-grade tumors. Cellular differentiation has also been used to grade salivary gland malignancies into well differentiated, moderately differentiated, poorly differentiated, undifferentiated, and anaplastic categories. Using this system, a significantly higher percentage of tumors in children (88%) are reported to be well differentiated or moderately differentiated in comparison with adults (49%).
Treatment of pediatric salivary gland neoplasms
The treatment of choice for most salivary gland neoplasms is complete removal of tumor with adequate margins. For submandibular tumors, complete excision of the gland is recommended. Parotidectomy is considered a safer and more definitive procedure than tumor enucleation, as the latter results in higher rates of recurrence and facial nerve dysfunction. Total parotidectomy is recommended for tumors with deep lobe involvement, suspected or confirmed high-grade tumors, or tumors with aggressive malignant potential such as those with facial nerve involvement, multiple intraparotid masses, or cervical metastasis. Definitive surgery allows for very good local control, with rates approaching 97% in some series.
Resection of the facial nerve is currently only recommended when there is gross anatomic or histopathologic evidence of neural invasion at the time of the surgery. When resection of the facial nerve is necessary, immediate reanimation by means of primary anastomosis or free nerve graft is advocated. Indications for neck dissection in adults with malignant salivary gland tumors include tumors larger than 3 cm, high-grade tumors, facial paralysis, extraglandular extension, and perilymphatic invasion. In children, some clinicians recommend simultaneous neck dissection at the time of primary tumor excision only when cervical nodal metastases are clinically detected. The clinical picture in children can be further complicated by lymph node hyperplasia, which is common, particularly in younger children, and may be mistaken for metastatic disease.
Postsurgical paresis/paralysis
Permanent facial nerve paresis or paralysis after surgery for benign parotid tumors in adults ranges from 3% to 5%, whereas transient facial nerve dysfunction ranges from 46% to 65%. These figures are notably higher when tumor enucleation rather than formal parotidectomy is undertaken. The risk of facial weakness may be greater in children than in adults, with one study reporting 10 of 21 cases having some facial nerve palsy. This risk is also higher in infants than it is in older children and in those undergoing total parotidectomy. Frey syndrome is characterized by hyperhidrosis and flushing of the lateral cervicofacial skin. These symptoms are due to abnormal skin innervation by the auriculotemporal nerve, which carries parasympathetic fibers that communicate with the sympathetic nervous system. Formal evaluation via a starch iodine test can reveal the presence of this syndrome in most postparotidectomy patients. In children, reports of Frey syndrome range from 0% to 47%. Children are typically managed expectantly. In adults, injection of botulinum toxin type A is the treatment of choice.
Postoperative radiation therapy for salivary gland malignancies
Postoperative radiation therapy has been shown to improve local and regional control of salivary gland malignancies in patients of all ages. The principal indications for radiotherapy include: high-grade malignancies, such as adenoid cystic carcinoma, squamous cell carcinoma, carcinoma ex pleomorphic adenoma, and undifferentiated carcinomas; gross or histopathologic evidence of perineural invasion or soft-tissue extension of tumor; multiple-level cervical lymph node metastases; and incomplete primary lesion resection. Children receive adjuvant radiation therapy less frequently than adults, owing to the higher risk of postradiotherapy complications (51% vs 27%) such as facial growth retardation and secondary malignant neoplasms. Intensity-modulated radiation therapy or proton beam therapy should be used in children whenever possible.
Chemotherapy is generally reserved for patients with progressive local or metastatic disease that is not amenable to surgery or radiation therapy.
Tumor recurrence
Tumor recurrence is reported in 7% to 20% of patients. Local and regional recurrence is more likely to occur in patients with positive margins, regardless of tumor grade. The 5-year overall survival for children with malignancies of the major salivary glands approaches 95%, in comparison with 59% for adults. Most tumors in younger patients are low-grade lesions, and these have an inherently better prognosis. Childhood salivary gland malignancies of the same stage and grade have outcomes similar to those of their adult counterparts. When tumor grades are examined in patients of all ages, 5-year survival rates range from 92% to 100% in cases of low-grade tumors, 62% to 92% for intermediate-grade tumors, and 0% to 43% for high-grade tumors. Poor prognostic factors include distant spread at diagnosis, development of second malignancies, male sex, high-grade tumors, large tumor size (>2.5 cm), perineural invasion, lymph node metastasis, soft-tissue extension, macroscopic residual disease, and pathologic diagnoses other than mucoepidermoid or acinar cell carcinoma.
Mucoepidermoid carcinoma
Mucoepidermoid carcinoma (MEC) is the most common primary salivary gland malignancy in adults and children. MEC accounts for approximately 30% of all epithelial carcinomas in patients of all ages, and represents up to 60% of all pediatric salivary gland malignancies. Macroscopically, MECs are firm, smooth, often cystic masses, which are tan, white, or pink in color with well-defined borders or infiltrative edges. Microscopically they are composed of epidermoid cells, mucous secreting cells, and intermediate cells ( Fig. 11 ). Several quantitative point-scoring grading schemes exist for MECs, including the Armed Forces Institute of Pathology grading system, the modified Healey system, and the Brandwein system. These systems assess characteristics such as intracystic components, the presence of neural invasion or necrosis, mitotic rate, and cellular anaplasia to stratify tumors into low, intermediate, or high grades. Most MECs in children are low grade, with relative frequencies of low (76%), intermediate (14%), and high (10%) grade.



